https://jasonpartin.com/wp-content/uploads/2019/09/buddha-meditating-meditation.jpg183275jasonpartinhttp://jasonpartin.com/wp-content/uploads/2019/03/logo-jp-jason-partin-cropped-50-px-high.pngjasonpartin2019-09-03 04:14:272019-09-30 18:52:25How to meditate
The Lonely Planet guide to India, the gold-standard of travel guides, a bible for budget backpackers, and usually a kind voice encouraging you to travel without judgement, said this about Varanasi India:
Brace yourself. You’re about to enter one of the most blindingly colorful, unrelentingly chaotic and unapologetically indiscreet places on earth. Varanasi takes no prisoners.
Varanasi tested my patience, humor, and immune system more than anywhere in the world, yet remains one of my favorite memories of a trip across Nepal and India.
https://jasonpartin.com/wp-content/uploads/2018/07/7c4f6e_f152faab6b0740839676bb8ecd125faamv2.jpg600800jasonpartinhttp://jasonpartin.com/wp-content/uploads/2019/03/logo-jp-jason-partin-cropped-50-px-high.pngjasonpartin2019-05-31 17:37:572019-06-06 02:17:09You get what you give in Varanasi India
Meditation and mindfulness reduce suffering from pain. The United States Veterans Administration advocates mindful awareness, a process each person must follow until finding what works for their unique situation. Many books and online resources are available to help your process; here’s what worked for me, I hope it helps you. Read more
https://jasonpartin.com/wp-content/uploads/2019/02/mindful.jpg500451jasonpartinhttp://jasonpartin.com/wp-content/uploads/2019/03/logo-jp-jason-partin-cropped-50-px-high.pngjasonpartin2019-05-31 16:30:242019-06-03 04:33:52Mindful meditation for pain relief
This article shares what I learned while meditating on the Buddha’s final words, while backpacking the route of his life from birth to death, from Nepal to India. Read more
https://jasonpartin.com/wp-content/uploads/2018/06/7c4f6e_b98cd9c6292a4de597ef6a6b840159bfmv2.jpg446640jasonpartinhttp://jasonpartin.com/wp-content/uploads/2019/03/logo-jp-jason-partin-cropped-50-px-high.pngjasonpartin2019-05-31 16:26:592019-06-03 04:34:32Meditate on the Buddha's final words
https://jasonpartin.com/wp-content/uploads/2019/03/7c4f6e_9c8c1daab72747489138c88d3c830200mv2-1.jpg8521049jasonpartinhttp://jasonpartin.com/wp-content/uploads/2019/03/logo-jp-jason-partin-cropped-50-px-high.pngjasonpartin2019-03-26 18:48:102020-01-04 21:34:58IIb, or not IIb: that is the question for the European Union Medical Device Regulation
Life should be fun, and I try to find ways to bring fun into work. This article uses Voltron, Defender of the Universe, to teach the European Union Medical Device Regulations requirements for Unique Device Identifiers.
https://jasonpartin.com/wp-content/uploads/2019/03/7c4f6e_a2fb9e2b472849dfac20e3c7443b3c4cmv2-1.jpg768862jasonpartinhttp://jasonpartin.com/wp-content/uploads/2019/03/logo-jp-jason-partin-cropped-50-px-high.pngjasonpartin2019-03-22 18:54:022020-01-04 21:35:45Learn the EU-MDR Unique Device Identifier System from Voltron
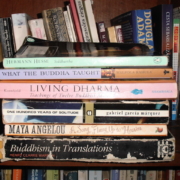
These are the lasting impressions of 30 books I read while backpacking across Nepal and India. The trip took 2 1/2 months; this summary takes a few minutes at the average reading rate of adults.
Books in English were rare treats shared between travelers, a chance to learn from other people including those who had been traveling your route dozens of years ago. Guest-houses in remote villages often had book-exchanges where people from all over the world shared books they had chosen to bring backpacking.
My first book swap was at a monastery in Kathmandu that used the $6/night from guests to fund a free healthcare clinic for Tibetan refugees. The exchange had books hundreds of travelers from all over the world had felt was worth carrying and sharing on their journeys. I read a few books about meditation during my week-long stay, left a copy of “One Hundred Years of Solitude,” and took a book on Buddhism to read during the next stage of my journey. That process continued for 2 1/2 months, resulting in a wide range of books I’ll summarize after introducing Deepak.
For over 35 years Deepak has sold books from a push-cart near the Tibetan University and Deer Park in Sarnath, India, where the Buddha gave his first sermon 2,600 years ago. It’s a pilgrim site for followers and students of Buddhism, Jainism, and Hinduism. Deepak’s calm, friendly, unassuming personality invites conversations about the books he carries; I was fortunate to spend two weeks getting to know him and reading books from his small but mindfully chosen selection of books.
Deepak has discussed books, religion, and philosophy with scholars, pilgrims, professors, and travelers for three decades. His ethos is Truth Prevails. I met him while waiting for a security clearance; I had been invited to attend a conference on Philosophy of the Mind and Modern Science, held in conjunction with the Tibetan University’s 50th anniversary. and attended by the Dali Lama, who had created the university after the Chinese army moved into Tibet and his people fled to India.
The conference included leaders from the religions represented in Deer Park to discuss different philosophies of the mind with scientists from all over the world working on topics ranging from neuroscience to physics. Most attendees hurried passed Deepak on their way to the conference each day, not realizing the wisdom held in his book cart.
Most of my memories from that conference are from Deepak’s books and our conversations about what people have been seeking since before the Buddha gave his first sermon 2,600 years ago. Few understand the goal, but the path is available to everyone: humility, patience, and perseverance. I was fortunate to not be in a hurry to the conference so that I could spend time with Deepak, learning from him and his books.
Before I left, Deepak invited me to meet his family and gave me a statue of the Buddha he had painted, hoping I could find space in my backpack to carry it home. Today, it’s on my bookshelf at home, reminding me of Deepak, a wise and kind person who helped me get a little wiser and a little kinder.
I continue to receive joy from the books and wisdom he shared, and will give my take-home impression from those books after a fun fact.
A Fun Fact
If you look at the book-exchange photo, you can see an author’s name, Douglas Adams, who wrote the book at the exchange”The Hitchhiker’s Guide to the Galaxy.” It’s about budget-backpacking in space using an electronic book similar to a Kindle e-reader, and has been one of my favorite books since reading it as a teenager.
The e-Guide to the Galaxy, which is similar to a travel guide to backpacking in remote countries, gives practical advice to travelers on it’s cover: “Don’t Panic.”
The photo below is Elon Musk’s convertible sports car, floating in space, facing the Earth, with a camera over the shoulder of a mannequin made to look like it’s driving the car. Elon Musk launched his car into space the day I started writing this blog. Elon is a fan of science fiction books, and if you look closely at his dashboard you’ll see his advice: “Don’t Panic”
I still enjoy this fact, especially while writing about finding a copy of the Hitchiker’s Guide to the Galaxy in a Tibetan Buddhist monastery in Nepal. Life if fascinating, fun, and often out of our control, so “don’t panic” is the practical advice to give anyone on any journey.
Vigorous writing is concise. A sentence should contain no unnecessary words, a paragraph no unnecessary sentences, for the same reason that a drawing should have no unnecessary lines and a machine no unnecessary parts. This requires not that the writer make all his sentences short, or that he avoid all detail and treat his subjects only in outline, but that every word tell.
Hinduism originated from a belief that there’s one god and that god is indescribable; Hindu deities are ways to comprehend the limitless aspects of a god.
The Buddha used the Hindu concept dukkha, which is approximately translated to “suffering” from obvious causes such as death, disease, and sadness but includes includes worry, anger, disappointment, impatience, judgement, or any unrest of the mind. Dukkha is anything other than experiencing a moment for what it is. My paraphrasing of the Buddha’s final words is:
“All I’ve taught is that there is suffering, the cause of suffering, suffering can end, and the path to end suffering is the middle way.”
All things created by the mind are impermanent. Practice your aim with diligence.”
Sudata’s biography: Born in Germany, defected from the Nazi army in WWII, wandered internationally to avoid prosecution, became a Buddhist monk, died peacefully.
Bhagavad Gita means “The Song of our Lord.” It’s a 2,500 year-old story about the god Krishna explaining older Hindu texts to a servant. It’s analogous to what the New Testament is to the Old Testament. My mind reacted negatively to the repeated message of “do your duty.”
When we hear about people suffering we become upset or worry, but do not do anything. We do not even wish them happiness. We may say the words, but we do not feel compassion, or we feel sadness and temporarily suffer with no benefit to anyone.
There’s a difference between memorizing physics and understanding it, or “seeing it.”
Before studying physics Einstein was interested in philosophy similar to Buddhist philosophy of the mind; Buddhist philosophy is based on understanding, not doctrine, so that people can “see things how they really are.”
A Buddhist philosophy is that wisdom comes from removing doubt rather than adding conviction. The mathematics of physics and results of modern experiments are ways to remove doubt about how things really are.
Humankind can see black holes by detecting Hawking radiation.
Stephen Hawking explains Classic & Quantum Physics using a vocabulary of a few hundred words. He wrote these books in his wheelchair, selecting letters and words from a computer screen by twitching his cheek. I think he sees things how they really are.
After 18 years of starting and stopping this book I came within 40 pages of finishing it. Other people have been more persistent; 100 Years of Solitude has more than 600,000 ratings and 22,000 reviews on Goodreads.com
The Buddha said, “Let a wise man watch his thinking. The mind moves with extreme subtlety and is not noticed. It seizes whatever it desires. To watch the mind is conducive to happiness.”
Data supports their claims, and they don’t claim more than data reveals.
I’d be interested in knowing how peoples’ actions impact the quality of their lives and the lives of others. A modern version of the Bell Curve could analyzes our actions, which are less debatable than our intelligence.
A lot of people have opinions about The Bell Curve.
I believe many people are reacting emotionally to a bigger problem that I would rather discuss: how to measure and improve happiness and social equity on a planet that will have 10 Billion people by 2050.
I carried both books in my backpack for months, including hiking over the Himalaya mountains in a heavy backpack. They facilitate traveling with an open mind.
Interesting, to me
I read “Bird of Passage” while staying in the guest house that the authors had stayed 17 years prior. I realized this while I was reading them describe the host’s cooking and watching the same owner prepare our dinner.
The guest-house host was the catalyst for me being invited to the first international conference on “Mind and Modern Science,” held at the Tibetan University and attended by the Dalai Lama for the University’s 50th anniversary, an auspicious visit because he had created the university after his exile from Tibet. At that conference I saw the Dalai Lama offer respect to Samdhong Rinpoche, the author of a book on Tibetan meditation that I coincidentally found at a coffee shop and summarized in this blog.
I taught physics, study religious philosophy, and enjoy American wild-west movies: In the Himalaya Mountains, I stayed at guest house that was decorated with physics posters, Buddhist art, and Clint Eastwood western-movie posters written in Dutch. It was the home of a Dutch physicist and his wife of twenty years, a Nepali Buddhist. They don’t receive many backpackers, and he was just as excited as I was to stay up all night discussing physics, philosophy, Buddhism, and how to make tasty homemade pasta.
Albert Einstein, Stephen Hawking, and Walpola Sri Rahula (when quoting the Buddha) use the words “relativity, space, and time” to describe concepts. Hawking and Rahula use the word “annihilation” when discussing something that ceases to exist in physical form. In other books by Einstein and Hawking they uses phrases that originated with the Buddha, 2,600 years ago. That had bothered me for years; I wouldn’t understand the root source until six months after returning from this trip and reading Einstein’s later essays and biography (I’m editing my original post with this information in August 2018, soon after reading Einstein’s essays). Einstein was influenced by the philosopher Schopenhauer who developed theories similar to Buddha’s, and Einstein would later discuss Buddha’s insights and compare them to his way of thinking. Einstein obviously influenced other physicists which may be why the words and way of speaking propagate. Plus, I believe the Buddha “saw” physics of the universe but didn’t have the words to describe them 2,600 years ago. He was too far ahead of his time, described things as best he could but admitted that words are limiting. The more I study what we know of his original words the more clear it becomes to me that he understood physics concept like the conservation of matter and atomic structure, but didn’t have the pre-existing language or tools to explain them. And, he was more focused on calming the human mind than teaching science; he created the phrase “conditioned genesis” to describe all phenomenon but only in the context of removing suffering from all humans. Today, we are just beginning to understand that all matter is a form of conditioned genesis, of particles being created and annihilated in a continuous process.
Post-Script
I published this blog in February 2018. In March 2018, Stephen Hawking died at age 76, more than 50 years older than he was expected to live when he was diagnosed with amyotrophic lateral sclerosis.
“I have lived with the prospect of an early death for the last 49 years. I’m not afraid of death, but I’m in no hurry to die. I have so much I want to do first”
“My advice to other disabled people would be, concentrate on things your disability doesn’t prevent you doing well, and don’t regret the things it interferes with. Don’t be disabled in spirit, as well as physically.”
He was able to train with astronauts in zero-gravity simulators, where the first rule is “don’t panic.” I’m happy every time I imagine the joy he must have experienced. Rest in Peace Professor Hawking.
Meditation and mindfulness reduce suffering from pain. The United States Veterans Administration advocates mindful awareness, a process each person must follow until finding what works for their unique situation. Many books and online resources are available to help your process; here’s what worked for me, I hope it helps you. Read more
https://jasonpartin.com/wp-content/uploads/2019/02/mindful.jpg500451jasonpartinhttp://jasonpartin.com/wp-content/uploads/2019/03/logo-jp-jason-partin-cropped-50-px-high.pngjasonpartin2019-02-17 19:38:412019-05-31 16:26:07Mindful meditation for pain relief